

Understanding the dosage interval of testosterone
Learn how your testosterone levels vary with different dosage intervals for injectable preparations like testosterone enanthate based on the pharmacokinetic profile.

Disclaimer: Mega Gonadal publishes information that is purely intended for educational purposes. Any action you take based on the information published in Mega Gonadal is taken at your own risk, and I cannot be held liable for any damages incurred. Remember that even though educating yourself is a good idea, consulting with a qualified medical professional is also a good idea. I cannot provide medical advice.

Summary (TL;DR):
Injecting testosterone preparations like testosterone enanthate once a week or once every two weeks leads to a roller-coaster of supraphysiological levels at the peaks and hypogonadal levels at the valleys.
Besides the roller-coaster of energy levels, this also runs the risk of throwing off your blood markers (e.g. rise of hematocrit and increased risk of erythrocytosis).
More frequent pinning leads to more stable levels, riding small waves instead of going on a roller-coaster, but doctors don’t favor more frequent pinning because they think patients won’t be okay with it.
When you’re injecting testosterone (this applies to other injectable androgens as well), it can be tricky to dial things if you don’t understand the pharmacokinetics of the drug (i.e. what your body does to the drug). Unfortunately, the standard clinical practice in this area is not the best practice to be following health-wise, in my opinion.
In this article, you’ll learn how to choose your dosage interval based on the pharmacokinetics of testosterone (or other androgens). After reading this article, you can decide for yourself which dosage interval suits you best based on your needs.
Single-dose pharmacokinetics
When you inject a testosterone preparation with a certain terminal half life, it absorbs, distributes, gets metabolized, and ultimate gets eliminated by your body. If you plot the serum concentration as a whole, you will see the concentration taking some time to reach a maximum as your body absorbs the drug, then the concentration slowly starts decreasing until you take your next shot, and the same thing happens again.
The pharmacokinetics of a testosterone preparation are determined by multiple factors, the most important of which are: the ester used, the vegetable oil solution used, the injection site, and the injection volume. In this article, we’ll only focus on the influence of the ester, but keep in mind that the pharmacokinetics are not solely determined by the ester.
We will focus on two testosterone preparations. The first is testosterone propionate which has a terminal half-life of only 0.8 day (this means that after every 0.8 day = 19.2 hours, the plasma testosterone concentration decreases to half what it was at the beginning). The second is testosterone enanthate, which has a longer terminal half-life of 4.5 days because the enanthate ester is longer than the propionate one, which means it takes longer to break it down. Note that the pharmacokinetic profiles presented here are found in academic studies that sadly don’t always provide information on the oil solution used for each testosterone preparation.
Let’s consider a single dose first. The following figure shows the pharmacokinetics of testosterone propionate. You can see how the plasma concentration reaches a peak in less than a day, then slowly decreases to very small levels by day 6. Notice how testosterone reaches supraphysiological peak levels at 40 nmol/L (= 1154 ng/dL) in less than a day, but by day 3, they’re already in hypogonadal territory at about 10 nmol/L (= 288 ng/dL).

Multiple-dose pharmacokinetics
In clinical practice, testosterone therapy using injectables favors preparations with a longer terminal half-life like testosterone enanthate rather than testosterone propionate. The “standard” dosage interval with intramuscular injections is once a week or once every two weeks. For example, the Endocrine Society’s guidelines set 75-100 mg for weekly injections or 150-200 mg every two weeks.
With intramuscular injections, after roughly 24 hours, the testosterone concentration reaches its maximum and then starts decreasing until the next shot a week later. The goal, of course, when it comes to testosterone therapy, is to achieve “physiological” levels, but because the dosage interval is so large, you end up having to inject a big amount every week to sustain your testosterone levels throughout the whole week until your next shot.
If you inject a reasonable amount, then the concentration will peak (after roughly 24 hours) in “supraphysiological” territory, with testosterone levels well above the so-called “normal” range. As the concentration decreases day after day, you will eventually end up in “hypogonadal” territory by the time you get around to taking your next shot, with clearly low levels of testosterone. On average, you will have stayed at a “normal” level, but the drop to hypogonadal levels toward the end of the week leads some people to favor injecting a higher amount so that they raise the tail end of the curve a little bit. This means, however, that they will be in even more supraphysiological at peak concentration.
Take for example the case of the previous preparation, testosterone propionate, with a terminal half-life of 0.8 day. The figure below shows the pharmacokinetics of a multiple-dose regimen (50 mg twice per week) for two weeks. The dashed lines show what might be considered the “normal” range of testosterone levels. The peaks are well above the upper limit and the valleys are well below the lower limit. The same thing is seen with testosterone enanthate at dosage intervals of once a week or once every two weeks.

Roller-coaster
The problem, as you can see, is that you go through a roller-coaster with supraphysiological levels in the first few days, decreasing to normal levels, and then finally to hypogonadal levels at the end of the week. Now, this doesn’t necessarily mean that you will feel the roller-coaster. Indeed, some people report feeling fine throughout the whole week, but a lot of people do notice how their energy levels seem to follow the roller-coaster. You can imagine how it’s even worse when the dosage interval is two weeks!
The problem with the roller-coaster is not just that you feel ups and downs. There is also a physiological problem with pinning a bolus amount of testosterone at once, which has the potential to throw off many markers in your blood, like your hematocrit for example. This is when there is a clear risk for erythrocytosis (producing an excess of red blood cells).
Because you introduce a bolus dose of testosterone at once, this means that its main metabolites (estradiol and dihydrotestosterone) will also rise to very high concentrations. You will thus also be exposing yourself to any negative effects that might be associated with “supraphysiological” levels of those two metabolites.
Doctors follow the practice of weekly injections because they believe that anything more frequent is unacceptable to patients. The idea is that people don’t like needles, and a lot of people have to go to a clinic to get their shot anyway because they don’t inject by themselves at home. Nevertheless, there are a lot of people who don’t mind pinning more frequently, and hopefully you’re one of them.
Frequent injections
A more frequent pinning schedule involves injecting smaller amounts more often, which means your levels will look more like small waves than a giant rollercoaster, which is obviously more ideal. The difference between the peaks and the valleys becomes much smaller than in the weekly regimen, and you are introducing smaller amounts of testosterone with every shot.
Pinning twice per week or every three days seems to be a good compromise between, on the one hand, achieving the benefits of more stable plasma concentrations, and on the other hand, the hassle of having to inject yourself, losing a little bit of oil with every shot, etc. Anything more frequent (every day or every other day) is excessive in my opinion and not necessary.
More frequent pinning is obviously the solution to achieving more stable physiological levels in the spirit of true testosterone “replacement”, but unfortunately, pharma research has gone the other direction, with focus on designing testosterone preparations with even longer half lives that require less frequent injections.
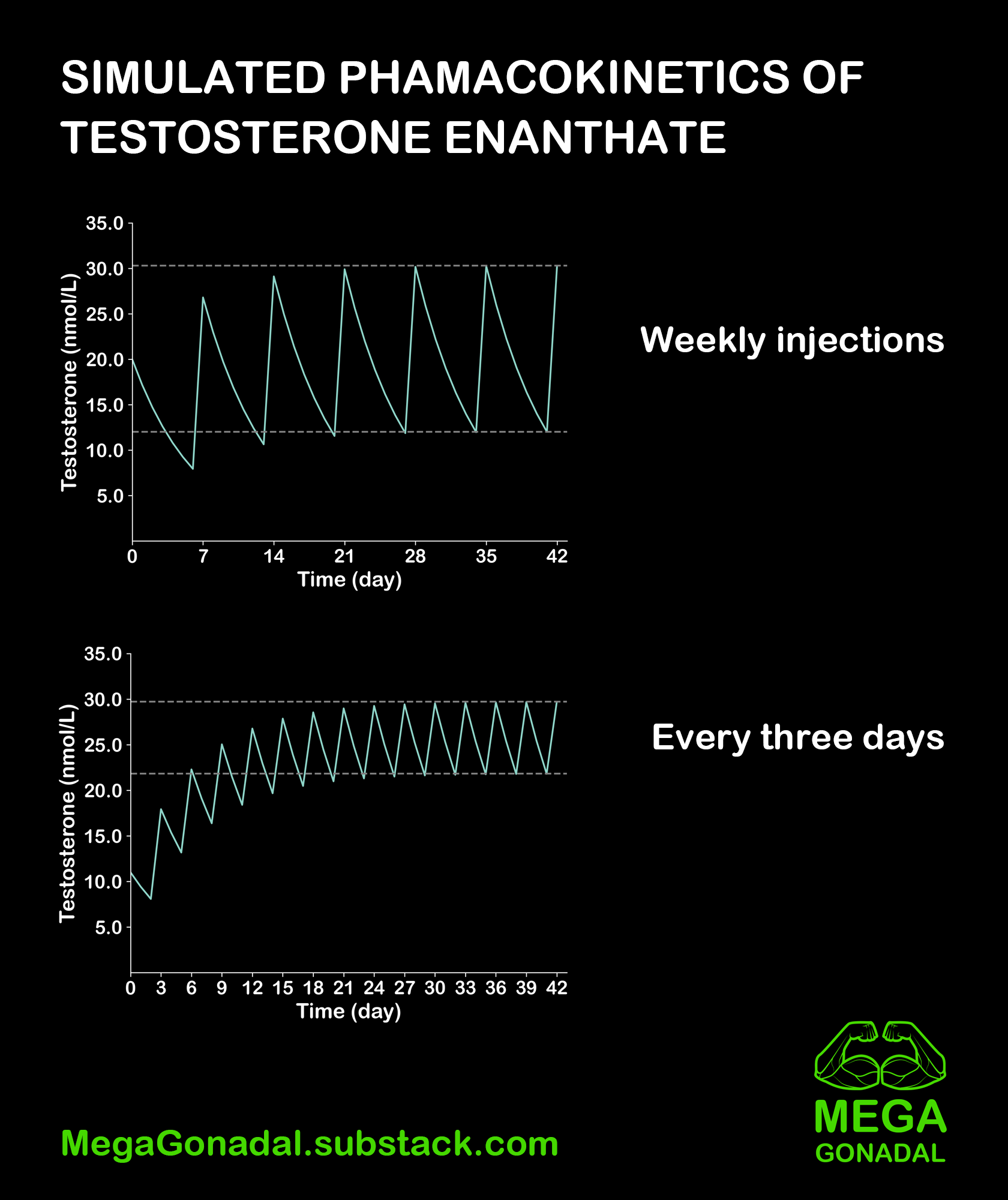
When you first start injecting, it takes a while for the testosterone to build up. After a few shots, you reach what is called “steady state”, which means that the testosterone at your dosage interval has saturated, and you’re now fluctuating between a maximum and a minimum that are pretty stable (assuming you’re consistent with your shots).
As you can see from the illustrations below, simulated weekly injections of testosterone enanthate (terminal half-life = 4.5 days) lead to a large difference between the steady-state minimum and maximum concentrations. A dosage interval of three days, however, leads to a minimum and maximum steady state concentrations that are much more similar, which is obviously more ideal.
Discussion
What do you think about dosage intervals for androgens? What is your preferred schedule for different compounds? Have you experimented with different intervals? What is your experience? Join the discussion by leaving a comment.